





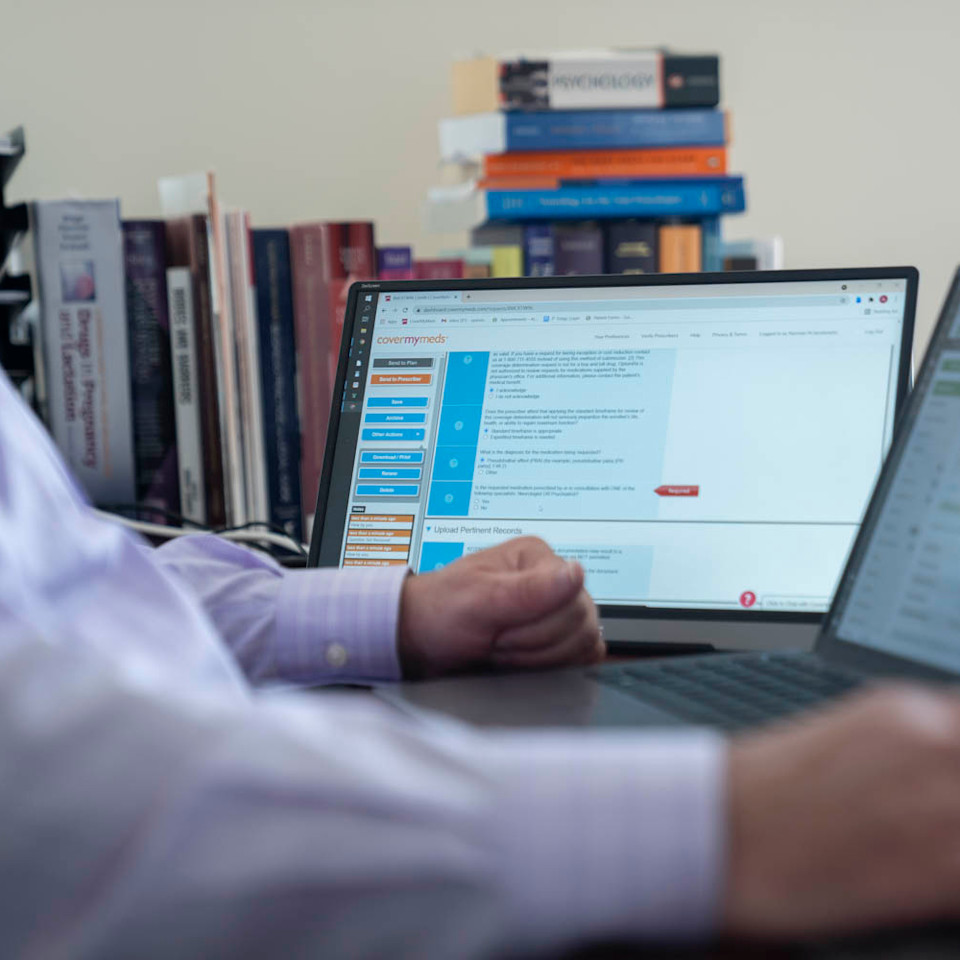
Norman Jacobowitz, CNP, manages his own psychiatry practice where he prescribes patients medication to treat conditions such as anxiety and post-traumatic stress disorder. Images by Ryan Donnell

Jacobowitz received very little training on the technology he uses. Many providers experience frustration with technology and administrative tasks, which can contribute to burnout in the profession.
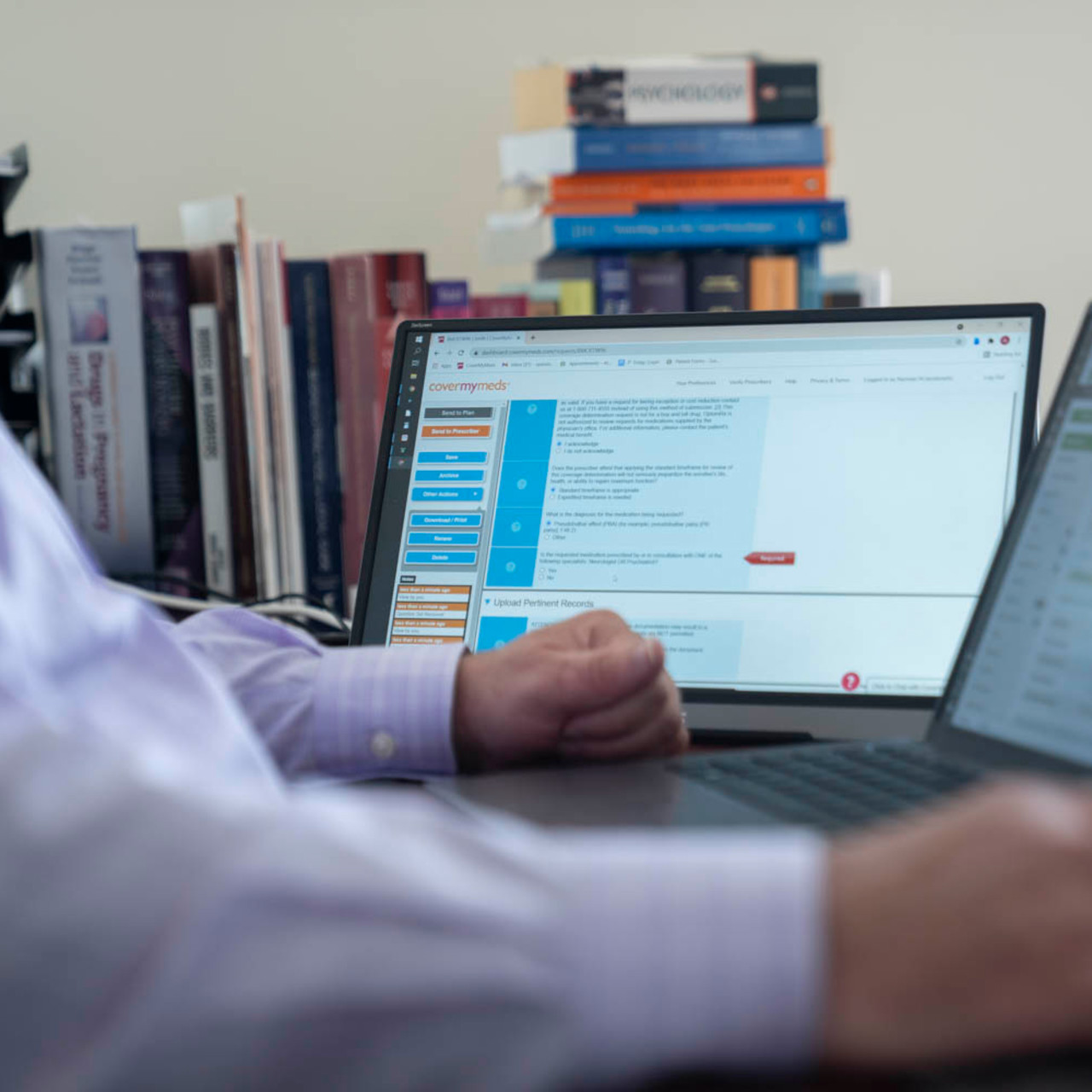
While provider ePA adoption is nearly universal, many providers and offices still use phone and fax for some PAs, due to varying requirements and uneven industry-wide adoption.
To fill information gaps in his technology workflow, Jacobowitz keeps a list of pre-written commands to save himself time. Integrated technology should surface all relevant prescribing information.
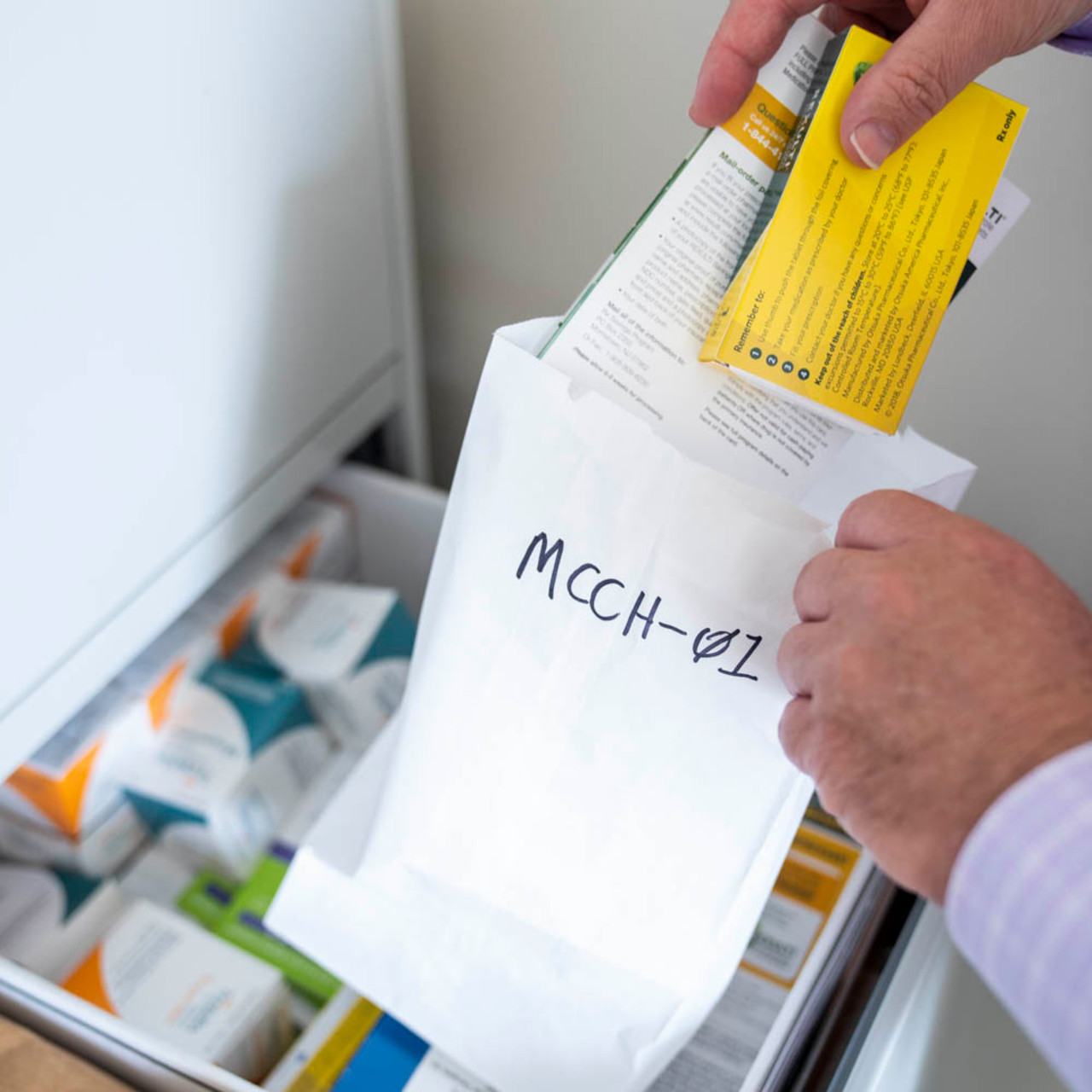
Jacobowitz knows many of the psychiatric drugs he prescribes come with a hefty price tag. He tries to find discounts and coupons for patients when he can and includes them in sample bags.

Providers like Jacobowitz balancing telehealth and in-person appointments critically need integrated, real-time solutions to help patients access, afford and adhere to medications.

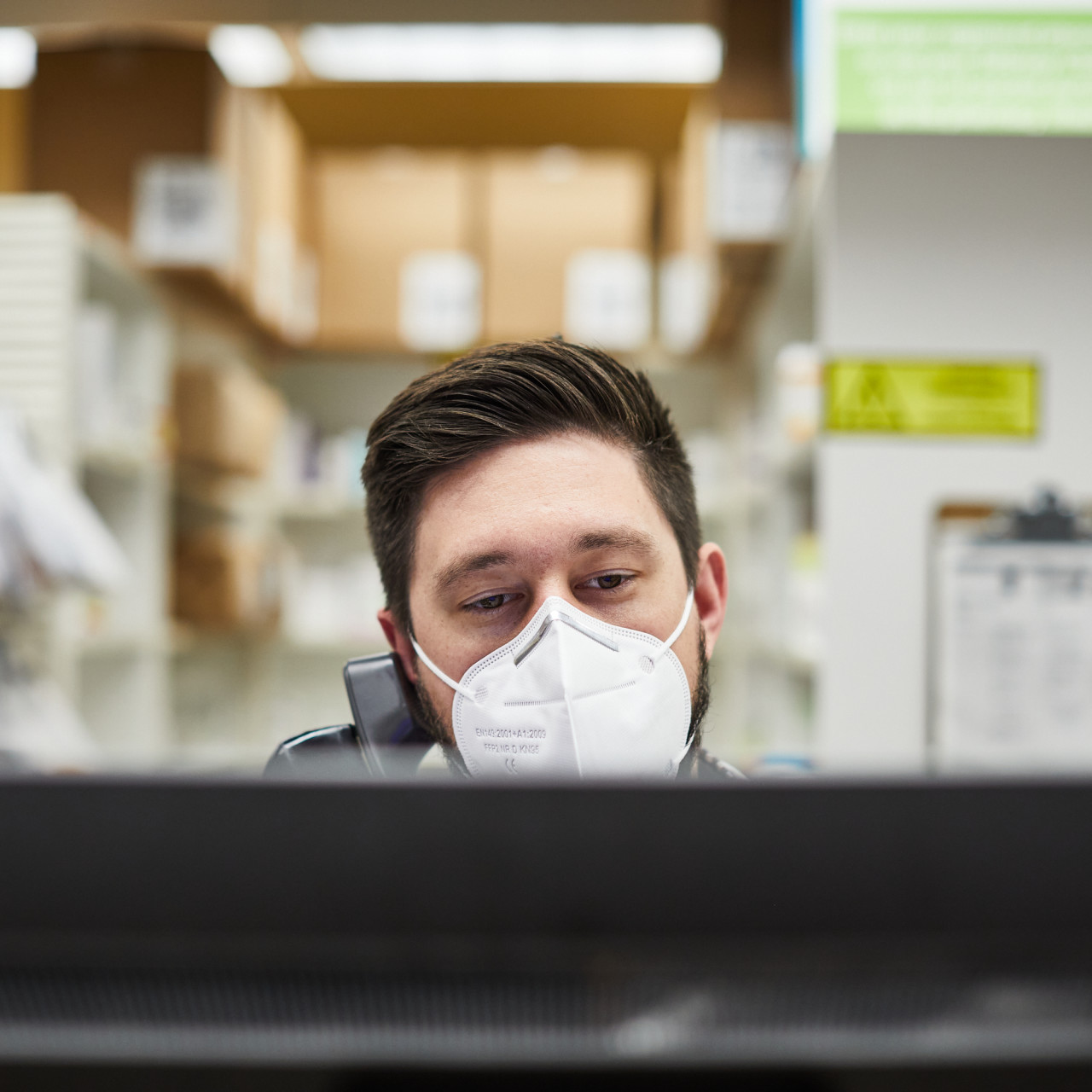
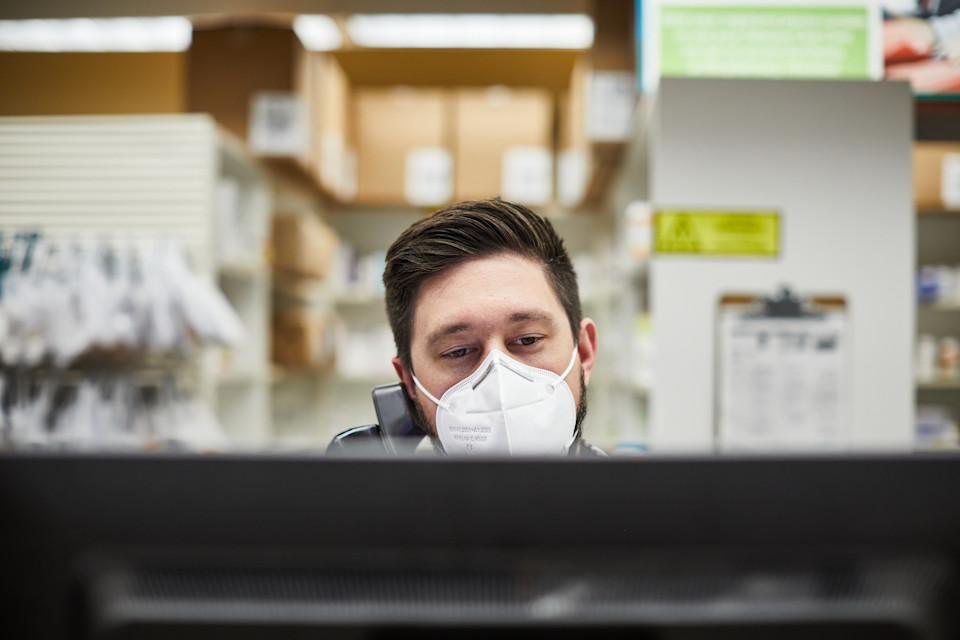
Gregory Hakala, Pharm.D, manages a large retail pharmacy and serves as a residency program coordinator for the Portland area. Images by Jay Fram

Technology can help give pharmacists time for clinical tasks such as administering vaccines to patients. Sixty-one percent of people preferred to receive their COVID-19 vaccine at a local pharmacy.

Hakala said there is most often only one pharmacist on duty during a shift to complete tasks that require this license - much of which occurs manually, outside their pharmacy system.
Only one-third of pharmacists surveyed receive PA updates within their pharmacy system. Most use phone and other time-consuming manual methods to communicate and manage PA requests.

Pharmacists using an integrated solution, inclusive of real-time PA status updates, see more paid claims, improving patient access to their medications.
Healthcare Technology
‘We’re still faxing. We’re still calling. We are now in 2021 … we should no longer be calling providers unless it’s 911.’
In this digital version of the 2021 Medication Access Report: Healthcare Technology Edition, we uncover care team pain points throughout the patient access journey and explore integrated, interoperable solutions for medication access, adherence and affordability.
For a deeper dive into medication access technology, download the 2021 Medication Access Report: Healthcare Technology Edition.
For Norman Jacobowitz, prescribing is an art, and he needs a better canvas.
A certified nurse practitioner, Jacobowitz runs his own psychiatry practice outside Washington, D.C. His workdays consist of diagnostic evaluation and medication management for a wide range of psychiatric conditions. When prescribing for these conditions, it’s more often a trial-and-error process than a transactional one.
“It really is artful, and there’s a lot of room for interpretation,” he said. “If you put 10 psychiatric providers in one room and present them with one case, you’re going to get 12 or 13 different opinions.”
Jacobowitz emphasized that gaining an understanding of patient goals — and their trust — helps him make better medication decisions with his patients. What sometimes gets in the way is outdated or clunky technology. This became a more intense pain point in the last year, as his practice contributed to the historic rise in telehealth visits due to the COVID-19 pandemic.
While psychiatry is a specialty more suited for telehealth than others, technology issues are condition-agnostic. Without face-to-face contact, Jacobowitz has no way to let patients know he’s having technology issues — because all communication relies on technology.


Usability impacts provider burnout
Like Jacobowitz, many providers experience an inefficient, disjointed workflow that can get in the way of the patient care experience. In a 2020 study, bureaucratic tasks and too many hours at work were major contributors to job burnout among providers, and nearly half of those surveyed said it has a severe impact on their life.National Physician Burnout & Suicide Report, Medscape, 2021 In some cases, physicians with burnout self-reported twice as many medical errors as those without.Physician Burnout, Well-being, and Work Unit Safety Grades in Relationship to Reported Medical Errors, Tawfik et. al., 2018
Improving the healthcare technology user experience can have a direct impact on burnout. When ranked on a standard system usability scale of 0 to 100, each additional point in an EHR’s usability was associated with a 3 percent lower chance of provider burnout.The Association Between Perceived Electronic Health Record Usability and Professional Burnout Among US Physicians, Melnick et. al., 2019
A major predictor of a positive user experience is proper technology training. Providers who received poor training were over 3.5 times more likely to say their EHR doesn’t allow them to deliver high-quality care.Local Investment in Training Drives Electronic Health Record User Satisfaction, Longhurst et. al., 2019 Jacobowitz said his training was next to nothing, but his previous IT experience gave him an edge in leveraging his current technology. Often, health systems and care teams are too busy to take time for technology training.
“I think at this point they rely on everybody (having) used some sort of EHR, and there’s enough congruence between them you can sort of jump from one to the other,” he said.

Providers need accurate, complete data
Even knowing a system backward and forward can’t help providers fill prescribing data gaps during and after patient appointments. Seventy-eight percent of providers report out-of-pocket costs are rarely or never available at the time of prescribing.CoverMyMeds Provider Survey, 2019 Of those who can surface this information in their EHR, most don’t trust it, including Jacobowitz.CoverMyMeds Provider Survey, 2019
“It’s frequently outdated,” he said. “I don’t know how accurate it can be. It does give me (benefit) information, but I don’t know where that’s coming from because I don’t have (patient) pharmacy benefit information in my system.”
To circumvent frustrating workflows and supplement lacking technology, Jacobowitz saved a list of macros, or simple computer commands, to better automate repetitive tasks such as sending medication instructions to pharmacists or patient relocation notices.
Interoperable, automated healthcare technology with complete datasets could improve provider frustrations and patient health outcomes. In one study, patients whose providers used prescription decision support technology inclusive of real-time benefit information were 19 percent more adherent to picking up their medication.CoverMyMeds data on file, 2019 Integrations such as real time prescription benefit (RTPB), electronic Prior Authorization (ePA) and even programs that surface drug-specific information within workflow help create a trusted technology experience for all care team needs — before, during and after prescribing.
RTPB and ePA can be time-savers for busy providers like Jacobowitz who said he sees up to 85 patients in a week. He’s not alone: Over half of providers surveyed said they don’t have the time they need to complete PA requests.CoverMyMeds Provider Survey, 2020 And while most have an electronic solution available, over half are still using manual methods like fax to submit at least some of them.CoverMyMeds Provider Survey, 2020 Jacobowitz said accessing an ePA portal is a non-negotiable part of his prescribing workflow, and he uses it at least a couple times a day.
“ePA has saved me an immense amount of time,” he said. “Other than my (EHR) it’s the second most common service I use.”
Real-time data can improve affordability conversations
As a specialist provider, Jacobowitz said he often has a good idea which payers will cover certain medications. What he can’t predict is his patients’ ability to afford them, with or without benefit coverage. In the last year, 43 percent of patients have stopped paying for bills or essential items to afford their medications; over one third gave up their medications to afford essentials.CoverMyMeds Patien Survey, 2020 These medication access conversations could impact a significant portion of the patient population. Tools within workflow that help surface affordability options can help providers lead the way, as 38 percent of patients said they won’t actively bring up these concerns.CoverMyMeds Patient Survey, 2020
In the case of psychiatry, an estimated three in four patients won’t find success with the first drug they try.Failure of First SSRI for Depression — What is the Next Step? Maoz, 2007
“There’s a lot of coping with the sometimes expected, sometimes unexpected negative side effects,” Jacobowitz said. “Sometimes you hit that med and the person’s doing great, but they’re having horrible side effects and you have no choice but to change it. The percent of patients you meet who fit into a nifty little category, you give them the med specific to the category and they get better is very low.”


Biopharma integrations can create better prescribing environments
Finding the right medication can be a confusing, expensive process, which is why samples and coupons from biopharma companies are critical to Jacobowitz’s practice. Unfortunately, due to the COVID-19 pandemic, fewer representatives are available to drop off samples, and telehealth can make it difficult to get these to patients. For some of his patients, Jacobowitz places the samples, along with a coupon if he has it, in a drop box outside his office with a patient-specific pickup code.
Biopharma information and coupons within a provider workflow could be a game-changer for patient conversations. Drug side-effects and interactions are complicated enough without getting into patient-specific coverage and cost details. Solutions that surface medication-specific details as well as easy-to-understand benefit information could also have a cumulative impact on patients’ health literacy.
In a recent study, only 50 percent of Americans could correctly define the word “deductible.”4 basic health insurance terms 96% of Americans don’t understand, PolicyGenius, 2018 Jacobowitz said many of his appointments often turn into education sessions on benefit details, medication information and what’s affordable.
“For most folks I say that drug is going to be expensive as a function of your deductible and ask, ‘Do you typically meet your deductible?’” Jacobowitz said. “Let’s think past the immediate sticker shock.”

Information captured at a specialist appointment, such as those with Jacobowitz, can be valuable to other patients’ providers, like their primary care physician. Interoperable systems that share patient history and results among health systems and providers could further promote elevated patient care and reduce duplicative care-team work. In a recent study, 81 percent of patients said they supported different healthcare providers sharing their health data among EHR systems.Pew HIT National Survey, PEW Charitable Trusts, 2020 APIs built to Fast Healthcare Interoperability Resource (FHIR) standards can help care teams avoid overwhelming amounts of data by pulling only the information they need instead of an entire record.
For larger practices and health systems, integration among various technologies specialized by position creates a delineated, connected workflow and can reduce the time it takes to track down information such as drugs on formulary, remaining deductible and medication history.
In many practices, while prescribers work with patients to make the final medication selection, nearly two-thirds of nurses said they’re influencing the prescription decision multiple times a week.CoverMyMeds Nurse Survey, 2019 They could avoid searching multiple places for this information — and aggregating it to share with the prescriber and patient — with a workflow inclusive of this information, integrated through direct pharmacy benefit manager (PBM), pharmacy and even biopharma connections.
Intelligent, automated systems early in the patient journey can further create efficiencies downstream when pharmacists enter the patient care continuum.
**Read more about integrated systems as a prescription for provider burnout in the full 2021 Medication Access Report: Technology Edition. **

Integrated pharmacy systems are critical to patient medication access
In the healthcare ecosystem, pharmacists can often feel like they’re stranded on remote islands, and communication to the mainland is usually limited to fax and phone calls — which, after days unanswered and hours on hold, may as well be messages sent in bottles.
Yet, for patients, pharmacists are one of the most accessible healthcare resources. Ninety percent of the U.S. population lives within 5 miles of a pharmacy.Exploring Accessibility of Community Pharmacy Services, Kelling, 2015 This patient accessibility goes beyond proximity, as many pharmacists were the easiest healthcare provider to get in front of over the last year. One in four patients said they’ve relied more on their pharmacist for information regarding their condition and medication due to the COVID-19 pandemic.CoverMyMeds Patient Survey, 2020

Pharmacies are also where 61 percent of people preferred to receive their COVID-19 vaccine.KFF COVID-19 Vaccine Monitor, Kaiser Family Foundation, 2021 Becoming a pillar of the patient care team is a welcome paradigm shift for pharmacists too. Gregory Hakala, Pharm.D., said a good day for him involves making medication recommendations to improve patient health, getting everyone the vaccines they need and ensuring his staff goes home on time.
Manual processes can increase time to therapy
This goal isn’t always easily achieved. Inefficiencies created through manual processes and resource shortages add up to a risk for adverse patient outcomes. In a recent survey of over 4,000 pharmacists, half said they don’t have adequate time to complete their job in a safe and effective manner.Pharmacist Workload Survey, State of Ohio Board of Pharmacy, 2021
To get ahead of these inefficiencies, Hakala studies labor models and future performance forecasts several months out so he can adequately staff the grocery-chain retail pharmacy he manages.
But some things remain out of his control, like technology — or the lack thereof. Hakala listed one of his staff’s biggest pain points as constant time on the phone. Most inbound calls, he said, are patient questions regarding prescription or prior authorization (PA) updates. Many of these could be answered through patient-facing applications, which many larger chains and retail pharmacies offer.
Adoption and use of patient apps are often stymied, especially for independent pharmacies, because pharmacists don’t have time to promote them or the apps don’t integrate complete sets of information, like patient-specific insurance and payment details. Jeremy Manchester, executive vice president of pharmacy system vendor Liberty Software, said pharmacy platforms should be completely oriented around the patient.
“One thing we’ve spent a lot of time on is technology that prevents extra work for the patient, (such as) making sure we gather all patients’ prescriptions, so they don’t have to make two trips,” Manchester said.

Care team members need in-workflow communication
Manchester also mentioned patient-pharmacist communication capabilities such as outbound voicemails that allow pharmacists to record and send voice messages to patients within their system, so they don’t have to spend time waiting on the phone. Two-way text messaging also allows quick, instant communication and allows patients to respond to messages.
“Patients have become very engaged in that,” Manchester said.
Most often, Hakala said, the outbound calls he and his staff make are attempts to contact provider’s offices to resolve medication issues — usually unsuccessfully.
“We’re using phones when we shouldn’t even be calling providers unless it’s 911 or an emergency issue,” Hakala said. “We’re still faxing, we’re still calling. Who knows if they got the fax? Who knows if someone threw it away? Who knows if someone forgot to tell the provider?”
Only half of pharmacists surveyed can stay within their electronic system to communicate with providers’ offices, while 90 percent are most often using the phone.CoverMyMeds Pharmacist Survey, 2020 Hakala allots about 30 minutes for each call to a provider’s office. Meanwhile, the work doesn’t stop.
“There’s only one pharmacist on duty usually, so while we’re on hold we also have to manage all the other six phone lines and patients picking up medications, getting vaccinations, counseling questions and whatever else arises,” Hakala said.
Leaving a message is always an option, but Hakala estimated providers’ offices return one out of every four of his pharmacy’s calls.
“It’s discouraging,” he said. “The biggest issue is we have no electronic communication with providers.”
Direct secure messaging has existed within provider-facing EHRs for years to allow provider-to-provider communication. This could also allow providers to communicate with pharmacists in a pre-established workflow, enabling quicker decisions and ultimately patients receiving their medications sooner.
Manchester said when considering healthcare tools and capabilities, technology organizations should bring pharmacists into the equation much earlier instead of retrofitting solutions to include the pharmacy as an afterthought.
When asked what communication capabilities would exist in their ideal tool, nearly 9 in 10 pharmacists listed electronic communication with providers as the most-selected answer.CoverMyMeds Pharmacist Survey, 2020 Right behind it is communication with insurance plans.CoverMyMeds Pharmacist Survey, 2020
Pharmacists are left to manage most PA Requests
Hakala said when medications require a PA request, they often submit the request, leave a message with the patient and cancel the prescription — otherwise, he said, it’s likely to never be filled. At times, over 100 prescriptions are paused, waiting on PA approval and potentially leaving pharmacies with a lot of money on the shelf at the end of the day.
“We're kind of left in the dark in the (PA) phase,” he said. “We get an email, but we don't have time to check emails. If it doesn't automatically go through, we just don't have time. PAs are the least of our concerns from our side because so many of them are unsuccessful.”
Electronic PA management isn’t enough when it comes to alleviating pharmacist workload — they need automation. Automated solutions, integrated within current workflows, can make a difference for both pharmacists and patients.


Eighty percent of pharmacists surveyed said staying within their pharmacy system is important to completing their jobs.CoverMyMeds Pharmacist Survey, 2020 Pharmacists using an integrated solution, inclusive of real-time PA status updates, saw an average 14 percent increase in paid claims, meaning more patients received their originally prescribed medication.CoverMyMeds data on file, 2019
Hakala also mentioned further integrations with payers and PBMs could include recommended solutions for rejected prescriptions, saving both pharmacists and providers time.
“We don't know the benefits of the patient,” Hakala said. “That's probably the biggest thing with technology and saving the patient money … is knowing when something rejects what possible solutions are.”
Pharmacists, care team members need complete patient history
For the most optimal healthcare ecosystem, Hakala said pharmacists should have access to a shared patient electronic medical record for seamless transitions of care, especially with patients with chronic diseases.
“Everyone is working off a different electronic system, everyone's trying to do it differently and nothing communicates seamlessly,” Hakala said. “I'd love to be able to pull up a patient’s chart and figure out why they are prescribed something, what they had been prescribed in the past and what type of reactions they had with it.
“Transitions of care is obviously a hot topic, but it will remain one until someone fixes it. It’s directly linked with the lack of information and communicating between providers.”

While many tools exist for the pharmacy, they’re not always integrated. And owners are often hesitant to adopt new technology because of the time and effort it would take in an already busy environment. Ideally, those creating pharmacy technology themselves, like Manchester, could help end users by making it nearly self-trainable and an improvement from manual processes — not another burden to shoulder.
“You have pharmacists working on the bench, doing bills, and for (them) to get (their) head wrapped around a new offering, that inertia becomes difficult,” Manchester said. “We have to make technology easy for them to use and low effort for them to adopt.”
These technologies can help automate administrative and manual processes so pharmacists like Hakala can continue practicing and helping improve patient lives.
“I love my job, actually,” Hakala said. “I’m doing something new every week … it keeps me passionate about my career.”
--
For a more comprehensive look at interoperable systems within the pharmacy and among the larger patient care team, read the 2021 Medication Access Report: Technology Edition.
--
Explore Other Sections


Press inquiries:
media@covermymeds.com
Advisory Board
The Medication Access Report is developed in consultation with an advisory board of healthcare experts representing major organizations across the industry — each with unique perspectives, interests and opinions.


